
Cellulitis Management for Lymphedema
Evidence-Based Care Including LVA for International Patients | Lymphedema Clinic Tokyo
This page is for international patients living with lymphedema and recurrent cellulitis accompanied by high fever (38.5°C or higher).
Based on peer-reviewed research and extensive clinical experience, Lymphedema Clinic Tokyo explains an evidence-based cellulitis management approach, including conservative care and lymphaticovenular anastomosis (LVA), which may help reduce the frequency of severe cellulitis and improve daily life.
Treatment of cellulitis, and suppression of onset by lymphatic venous anastomosis
Lymphedema and cellulitis
It is thought that about 30% of lymphedema patients develop cellulitis. The affected area suddenly reddens, followed by rapid progression, with a fever of 39-40℃ developing within several hours. If items 1 to 3, below, are all found, the probability of cellulitis is high:









- 1Redness in the lymphedema region.
- 2The red area feels hot when touched.
- 3High fever (sometimes absent).
It is generally thought that cellulitis develops if bacteria enter a wound. However, in the case of patients with lymphedema, cellulitis develops even without injuries, irrespective of how much care the patient takes. It frequently occurs around the New Year, in early summer, or when patients are particularly busy at work.
If cellulitis occurs repeatedly, it becomes difficult for patients to travel or be involved with their hobbies and interests, etc. In addition, cellulitis may damage the lymphatic vessels and/or make the lymphedema worse. Patients who repeatedly suffer from cellulitis are therefore recommended to undergo appropriate treatment as soon as possible.
Cellulitis treatment
If people who develop cellulitis are able to drink liquid and eat meals, they often recover as a result of treatment at home, without hospitalization. However, if patients find it difficult to drink water due to high fever, or have a continuous high fever, it is often better for them to be hospitalized. Please consult the internal medicine and/or dermatology department at an emergency or general hospital, or your cancer primary-care physician, to decide whether this applies to you.
- 1Rest:While you have a fever, you should rest and conserve your energy.
- 2Antibiotics:These should be prescribed for you by the internal medicine or dermatology department.
- 3Cooling:This is an important aspect of treatment. You should cool the part of your body that has turned red. Roll a bag containing ice water backward and forward on the red, swollen area. This should alleviate the redness and swelling. Note that excessive cooling of a single site can lead to frostbite, so the bag must be rolled evenly, and not kept on a single spot. Alternatively, you can put a wet towel in a plastic bag, and place this on the red area.
*Compression therapy:Edema may be more severe than usual when cellulitis is present, and the usual compression stockings and sleeves may therefore not be appropriate. Pain also sometimes occurs due to inflammation. In such cases, compression therapy can be temporarily suspended. When the pain abates, alleviation of edema can be achieved by starting compression therapy again. However, compression stockings and sleeves can easily cut or work their way into the flesh, and more care than usual is therefore necessary.
*Massages:When redness is present, massages should be avoided.

Cellulitis prevention
Can Recurrent Cellulitis in Lymphedema Be Prevented?
— Evidence-Based Use of Prophylactic Antibiotics and LVA Strategy —
Recurrent cellulitis with high fever is one of the most distressing complications for patients living with lymphedema, often limiting daily life, work, and travel.
This page introduces a high-quality Cochrane systematic review showing that prophylactic antibiotics can significantly reduce cellulitis recurrence during the treatment period, and explains how we integrate this evidence into our clinical practice.
We present our stepwise, individualized strategy, combining conservative care, lymphaticovenular anastomosis (LVA), and time-limited antibiotic use, aiming to reduce cellulitis risk while avoiding unnecessary long-term medication.
Living with lymphedema is already challenging.
For many patients, recurrent cellulitis with high fever becomes an additional and deeply distressing burden.
You may have experienced:
・Sudden high fever and chills
・Painful redness and swelling of the affected limb
・Emergency hospital visits or intravenous antibiotics
・Anxiety about travel, work, or daily activities
・Constant fear of “when it might happen again”
These experiences can significantly affect quality of life, independence, and emotional well-being.
You are not alone—and importantly, recurrent cellulitis is not something you must simply endure.
【What Does Medical Evidence Tell Us About Prevention?】
To better understand how cellulitis recurrence can be reduced, we rely on high-quality international medical evidence.
A Cochrane systematic review, one of the most trusted forms of medical research, analyzed multiple randomized controlled trials involving adults with recurrent cellulitis.
This review showed that:
・Prophylactic (preventive) antibiotics significantly reduce cellulitis recurrence while the medication is being taken
・The benefit is seen during the treatment period
・The protective effect does not necessarily persist after antibiotics are stopped
This means that antibiotics can be effective as a temporary protective measure, but they should be used thoughtfully and strategically—not indefinitely.
【How We Integrate This Evidence Into Our Clinical Practice】
At our clinic, we believe that cellulitis prevention should be individualized, stepwise, and time-limited.
Our approach is based on three pillars:
1. Conservative Care as the Foundation
We emphasize meticulous skin care, compression therapy, and early treatment of minor skin injuries or fungal infections.
Healthy skin is the first line of defense against cellulitis.
2. Addressing the Underlying Lymphatic Problem
When conservative care alone is not enough, we consider surgical options such as:
Lymphaticovenular anastomosis (LVA)
Other lymphatic procedures tailored to the patient’s condition
By improving lymphatic drainage, we aim to reduce the biological environment that allows infections to occur repeatedly.
3. Thoughtful, Time-Limited Use of Antibiotics
Antibiotics are not intended as lifelong medication.
In our practice:
・Preventive antibiotics may be used during high-risk periods, such as before or after surgery
・Once the condition stabilizes, antibiotics are gradually reduced and discontinued
After discontinuation, short-term antibiotics (typically 2–3 days) may be used only when risk temporarily increases, such as during:
・International travel
・Periods of severe fatigue or sleep deprivation
・High physical or emotional stress
This strategy helps balance infection prevention and antibiotic safety.
【Why We Do Not Recommend Lifelong Antibiotics】
Some patients worry about:
・Antibiotic resistance
・Long-term side effects
・Dependency on medication
These concerns are valid.
Medical evidence—including the Cochrane review—supports the idea that antibiotics should be used when they provide benefit, and stopped when they no longer do.
Our goal is to protect you when needed, and reduce medication when it is safe to do so.
【Cellulitis Prevention Is About Protecting Your Life, Not Just Treating Infection】
Preventing cellulitis means more than avoiding hospitalization.
It means:
・Feeling safe to travel
・Being able to work and exercise with confidence
・Sleeping without fear of sudden fever
・Regaining control over your daily life
We believe that cellulitis prevention is an essential part of comprehensive lymphedema care.
【For Patients Considering Visiting Our Clinic from Overseas】
We understand that traveling internationally for medical care requires trust, clarity, and reassurance.
Our team:
・Treats a large number of patients with lymphedema and recurrent cellulitis
・Combines evidence-based medicine with individualized clinical judgment
・Carefully coordinates conservative care, surgery, and medication
・Communicates clearly with international patients before, during, and after treatment
While outcomes vary from person to person, our goal is always the same:
to help you live with greater stability, safety, and peace of mind.
【Reference (Accessible to Patients)】
Interventions for the prevention of recurrent erysipelas and cellulitis
Cochrane Database of Systematic Reviews
This internationally recognized review forms an important scientific basis for our approach.
Frequently Asked Questions(FAQ)
Recurrent Cellulitis in Lymphedema – Evidence-Based Prevention
Q1. What is cellulitis, and why is it so common in patients with lymphedema?
Cellulitis is a bacterial infection of the skin and subcutaneous tissue.
In patients with lymphedema, lymphatic flow is impaired, which makes it easier for bacteria to enter and spread.
As a result, cellulitis may occur suddenly with high fever, redness, swelling, and pain, and it often tends to recur.
Q2. Is recurrent cellulitis something I must live with forever?
No.
Recurrent cellulitis is not simply an unavoidable consequence of lymphedema.
High-quality medical studies show that, in selected patients, appropriate preventive strategies can significantly reduce recurrence, especially during high-risk periods.
Q3. What does medical research say about preventing recurrent cellulitis?
A well-known systematic review published in the Cochrane Database of Systematic Reviews analyzed randomized controlled trials in adults with recurrent cellulitis.
The review showed that:
・Prophylactic (preventive) antibiotics reduce cellulitis recurrence while they are being taken
・The protective effect is mainly seen during the treatment period
・The effect does not always continue after antibiotics are stopped
This means antibiotics can be helpful, but they should be used strategically, not indefinitely.
Q4. Does this mean I need to take antibiotics for the rest of my life?
No.
Long-term or lifelong antibiotic use is not recommended.
In our practice, antibiotics are used:
・Only when the risk of cellulitis is high
・For limited periods of time
・With a clear plan for dose reduction and discontinuation
The goal is protection when needed, and freedom from unnecessary medication when possible.
Q5. How does your clinic use antibiotics differently?
We use antibiotics as part of a stepwise, individualized strategy, not as a standalone or permanent solution.
Typically:
・Preventive antibiotics may be used during high-risk phases, such as around surgical treatment
・Once the condition stabilizes, antibiotics are gradually tapered and stopped
・After discontinuation, short-term antibiotics (2–3 days) may be used only when temporary risk increases, such as:
→International travel
→Severe fatigue or sleep deprivation
→Periods of intense physical or emotional stress
Q6. How does surgery, such as LVA, relate to cellulitis prevention?
Surgery such as lymphaticovenular anastomosis (LVA) aims to improve lymphatic drainage itself.
By addressing the underlying lymphatic dysfunction:
・The local environment becomes less favorable for infection
・The frequency and severity of cellulitis episodes may decrease
・Dependence on antibiotics may be reduced over time
Surgery is not required for every patient, but can be an important option for selected cases.
Q7. Why not rely on antibiotics alone?
Because cellulitis in lymphedema is not only about bacteria—it is also about lymphatic dysfunction and skin vulnerability.
Antibiotics alone do not correct the underlying lymphatic problem.
That is why we combine:
・Skin care and compression
・Lymphatic surgery when appropriate
・Time-limited antibiotic use
This comprehensive approach aims for long-term stability, not just short-term infection control.
Q8. What about antibiotic resistance and side effects?
These are valid concerns.
To minimize risks:
・Antibiotics are prescribed only when truly needed
・Treatment duration is kept as short as safely possible
・Long-term continuous use is avoided
This approach helps balance infection prevention and antibiotic safety.
Q9. If I feel early symptoms of cellulitis, what should I do?
Early action is crucial.
If you notice:
・Increasing redness, warmth, swelling, or pain in the affected limb
・Fever, chills, or sudden fatigue
You should follow the emergency guidance provided by our clinic and seek medical evaluation promptly.
Early treatment can often prevent severe infection or hospitalization.
Q10. How does cellulitis prevention improve quality of life?
Preventing cellulitis means more than avoiding infection.
It often allows patients to:
・Travel with confidence
・Maintain work and daily activities
・Exercise without fear
・Live without constant anxiety about sudden fever
For many patients, cellulitis prevention is a key step toward regaining control over daily life.
Q11. Is this approach suitable for international patients?
Yes.
We regularly care for patients traveling from overseas and understand the additional concerns involved.
Our team:
・Provides clear explanations before treatment
・Plans care efficiently for limited stays in Japan
・Offers guidance for long-term management after returning home
All treatment decisions are made individually, based on your condition and circumstances.
Q12. Where can I read the original research myself?
You may refer to the following publication:
Interventions for the prevention of recurrent erysipelas and cellulitis
Cochrane Database of Systematic Reviews
This internationally recognized review provides the scientific foundation for our preventive strategy.
Emergency Action Checklist
【Fever & Suspected Cellulitis (for Patients with Lymphedema)】
If you live with lymphedema, a sudden fever can feel frightening—especially when you are far from your medical team.
This checklist is designed to help you act early, stay safe, and reduce the risk of severe infection.
Important: This guide is for suspected cellulitis associated with lymphedema. It does not replace urgent medical evaluation. If symptoms are severe or rapidly worsening, seek emergency care immediately.
【1) Recognize the Early Warning Signs】
A. Limb/skin signs (often appear first)
・New or spreading redness
・Warmth/heat in the skin (hot to the touch)
・Increasing swelling or tightness compared to your usual baseline
・New or worsening pain/tenderness
・Skin feels “stretched,” shiny, or unusually sensitive
B. Whole-body signs (often indicate progression)
・Fever (especially ≥ 38.5°C / 101.3°F)
・Chills or shaking
・Strong fatigue or “flu-like” feeling
・Headache, body aches, loss of appetite
C. Possible entry points for bacteria
・Cuts, cracks, dry skin, eczema flare
・Athlete’s foot / fungal infection between toes
・Insect bites, shaving nicks
・Needle punctures, cat/dog scratches
If you notice limb changes + fever or chills, treat it as urgent.
【2) Check Your Temperature and Document Symptoms (takes 2 minutes)】
✅ Do now
・Measure and write down your temperature
・Take a photo of the affected area (good lighting)
・Mark the edge of redness with a pen (if possible) and note the time
・Write down:
→When symptoms started
→Whether redness is expanding
→Any recent skin injury, travel, overwork, or sleep deprivation
These details help clinicians make decisions faster.
【3) Decide the Level of Urgency (Simple Triage)】
A) Go to the Emergency Department / Call Emergency Services NOW if:
・Temperature ≥ 39.0°C (102.2°F) OR severe chills/rigors
・Rapidly spreading redness (expanding over hours)
・Severe pain, confusion, fainting, shortness of breath
・You cannot keep fluids down, or you feel dangerously weak
・Purple/black discoloration, blisters, or severe skin breakdown
・You are immunocompromised (e.g., chemotherapy, high-dose steroids) and have fever
Do not wait. Severe cellulitis can escalate quickly.
【B) Seek urgent medical evaluation within the same day if:】
・Fever ≥ 38.5°C (101.3°F) with limb redness/warmth/swelling
・Fever is rising even if limb changes seem mild
・The limb feels significantly more painful or tense than usual
・You have a history of recurrent cellulitis and symptoms are familiar
【C) Monitor closely and contact your clinic if:】
・No fever yet, but new localized redness/warmth is appearing
・You feel “off” (fatigue, mild chills) and limb symptoms are developing
・You are unsure—when in doubt, treat it as urgent
【4) If Our Clinic Has Given You a “Standby Medication Plan” (Very Important)】
If you have already been instructed by our clinic to keep specific medications at home:
✅ Follow our instructions exactly regarding:
・Antibiotics
・Antipyretics (fever reducers)
🚫 Do not:
Change the dose on your own
Stop early because you feel better
Switch to a different antibiotic without medical guidance
If you are unsure what to take, seek medical evaluation first.
【5) Support Your Immune System Immediately (What to Do Today)】
When cellulitis is suspected, your body needs rest.
✅ For the next 24–72 hours
・Increase your sleep time by about 1 hour compared with your usual routine
(Even one extra hour of sleep can support immune function and recovery.)
・Cancel strenuous exercise and avoid overwork
・Hydrate (water, oral rehydration solution if needed)
・Eat gentle, easy-to-digest foods if you can
・Keep the room comfortably warm
This is not “being weak.” It is medical self-care.
【6) Limb Care During Suspected Cellulitis (Safety First)】
✅ Generally recommended
・Rest the affected limb
・Keep skin clean and dry
・If walking is painful, reduce weight-bearing and use support
⚠️ Compression garments/bandaging
・If compression causes significant pain, numbness, or worsening discomfort, remove it and seek medical advice.
・If you are unsure, prioritize medical evaluation—especially with fever.
🚫 Avoid
・Aggressive massage or strong manual drainage when fever is present
・Hot baths/sauna (can worsen inflammation and dehydration)
・Scratching the area, shaving over irritated skin
【7) What to Tell the Doctor / ER (Copy-Paste Script)】
You can show this to clinicians:
“I have lymphedema and I suspect cellulitis. I have fever and new redness/warmth/swelling in the affected limb. I have a history of recurrent cellulitis. Please evaluate me for cellulitis and advise on antibiotics and whether IV treatment is needed.”
Also mention:
・Allergies to antibiotics
・Your current medications
・Any recent surgery, travel, injury, or fungal infection
【8) After the Acute Episode: Preventing the Next One (Once You’re Stable)】
When fever is gone and you are recovering, prevention matters.
✅ Key prevention steps
・Skin care: moisturize daily, treat cracks promptly
・Manage fungal infections (especially feet)
・Continue appropriate compression and lymphedema care
・Discuss long-term strategy (including surgery options such as LVA, if appropriate)
If you experience repeated episodes, a structured plan can reduce recurrence.
【9) Link: Our Emergency Guidance Page】
For our clinic’s official guidance and next steps, please refer to:
Emergency Response (Fever / Suspected Cellulitis)
Gentle Reminder
If you are reading this while anxious or unwell:
You are doing the right thing by seeking information early. Cellulitis is treatable, and early action can make a big difference.
【Frequently Asked Questions(FAQ)】
For International Patients Considering Treatment at Our Clinic
Q1. I live overseas. Can I still receive support from your clinic after returning home?
Yes.
After online consultation and also after LVA surgery, we continue to provide free email-based follow-up support, even after you return to your home country.
If you experience:
・anxiety or uncertainty
・questions about symptoms
・concerns about fever or cellulitis
・questions about daily care after surgery
please feel free to contact us at any time.
When necessary, we are also happy to communicate with your local doctors or therapists to coordinate care, so that you are not managing your condition alone after returning home.
Q2. How long do I need to stay in Japan for treatment?
In most cases, the total stay in Japan is approximately two weeks.
This period typically includes:
・preoperative evaluation
・LVA surgery
・postoperative observation and guidance
We also provide a separate page with example schedules to help you understand what daily life during your stay may look like.
Please refer to that page for practical planning.
Q3. Can LVA surgery really help prevent recurrent cellulitis with high fever?
Medical evidence suggests that LVA surgery can significantly reduce the frequency of severe cellulitis, especially cellulitis accompanied by high fever (≥38.5°C / 101.3°F).
In our published research:
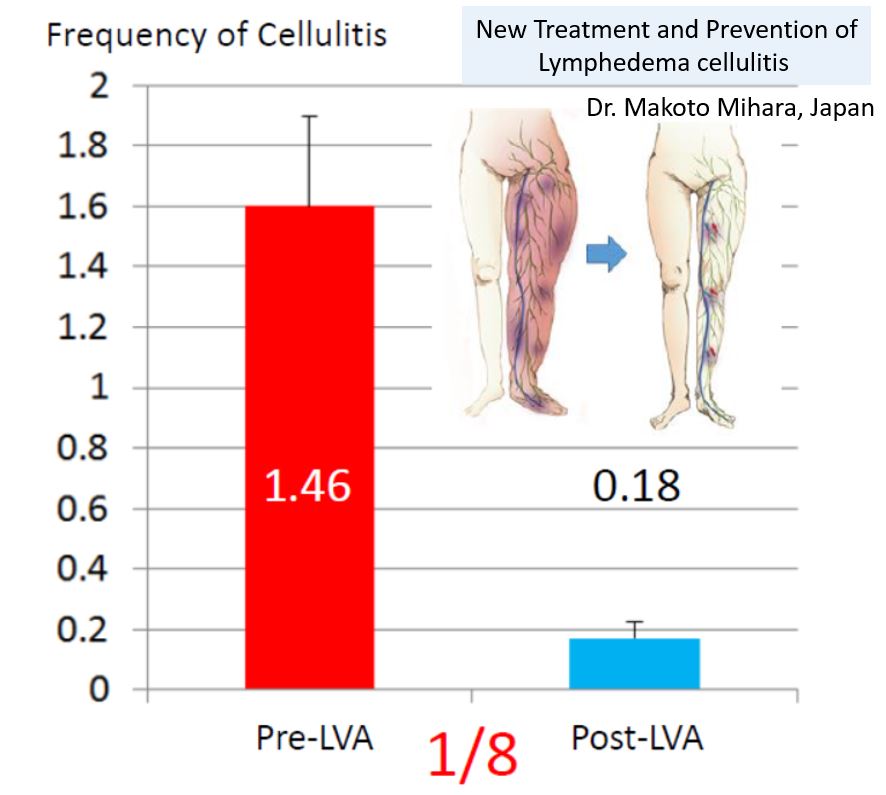
・A single LVA procedure was associated with a reduction in severe cellulitis episodes to approximately one-eighth of the previous frequency
・After one surgery, about 80–90% of patients experienced clear symptom improvement
These results are based on peer-reviewed scientific publications.
However, outcomes vary depending on individual condition and disease severity.
Q4. What if cellulitis continues even after LVA surgery?
A small proportion of patients (approximately 10–20%) may continue to experience recurrent cellulitis even after initial LVA surgery.
In such cases:
・We carefully reassess lymphatic anatomy
・Additional, carefully planned LVA procedures may be considered
Based on our clinical experience, with stepwise and meticulous additional surgery, more than 99% of patients treated at our clinic eventually experience meaningful improvement, with a marked reduction in severe, high-fever cellulitis episodes.
Again, individual outcomes may vary, but persistence does not mean failure—it means refinement of treatment.
Q5. If cellulitis occurs after LVA surgery, is it still severe?
In many patients, cellulitis episodes become much milder after LVA surgery.
Compared to before surgery:
・Fever may remain in the 37°C range rather than high fever
・Symptoms often resolve within 2–3 days
・Hospitalization is often unnecessary
・Many patients are able to continue work or daily activities
This change alone can dramatically reduce fear and disruption to daily life.
Q6. What should I do if cellulitis occurs after surgery?
If cellulitis occurs after surgery, we usually recommend:
・Short-term oral antibiotics (2–3 days), following prior instructions
・Increasing sleep time by about one hour, to support immune function
・Reducing physical and mental stress temporarily
We will guide you by email if needed, even after you have returned to your home country.
Q7. Will I need to take antibiotics long-term after surgery?
No.
Our approach does not involve lifelong or continuous antibiotics.
Antibiotics are used:
・strategically
・for limited periods
・only when the risk of cellulitis is temporarily increased
The goal is to reduce infection risk while minimizing unnecessary medication exposure.
Q8. I am worried about traveling internationally for surgery. Is this common at your clinic?
Yes.
We regularly care for patients traveling from overseas and understand the concerns involved, including:
・limited time in Japan
・language barriers
・post-return medical support
Our system is designed to provide:
c・lear pre-visit planning
・efficient in-country care
・ongoing remote follow-up after you return home
You will not be “on your own” once you leave Japan.
Q9. Is LVA surgery suitable for everyone with lymphedema and cellulitis?
Not necessarily.
LVA surgery is considered based on:
・lymphatic imaging findings
・frequency and severity of cellulitis
・response to conservative therapy
・overall health status
This is why online consultation and detailed evaluation are essential before making any decision.
Q10. What is the main goal of your approach for international patients?
Our goal is not only to treat infection, but to help you:
・live with greater stability
・travel without constant fear of fever
・continue work and daily life
・regain confidence and peace of mind
Cellulitis prevention is not just about medicine—it is about restoring quality of life.
- 1Compression therapy should be reconsidered.
- 2Surgery:Lymphatic venous anastomosis
- 3Surgery:Genital lymphatic vesicle resection (if genital lymphatic vesicles are present)
- 4Long-term, oral antibiotic administration
If the appropriate compression therapy is provided, involving elastic stockings, bandages, etc., cellulitis often does not develop. However, if you are currently not confident about undergoing compression therapy, you feel that compression therapy is not sufficiently effective, and/or a mark remains after pressing the affected area with a finger, you should consult a physician whose specialty is lymphedema. If you reconsider compression therapy, it is sometimes possible to alleviate edema, and to hinder the onset of cellulitis. If there are no physicians who can provide the appropriate treatment in your country, you can be treated at our clinic. We will make the appropriate diagnosis, and then present you with a treatment proposal.
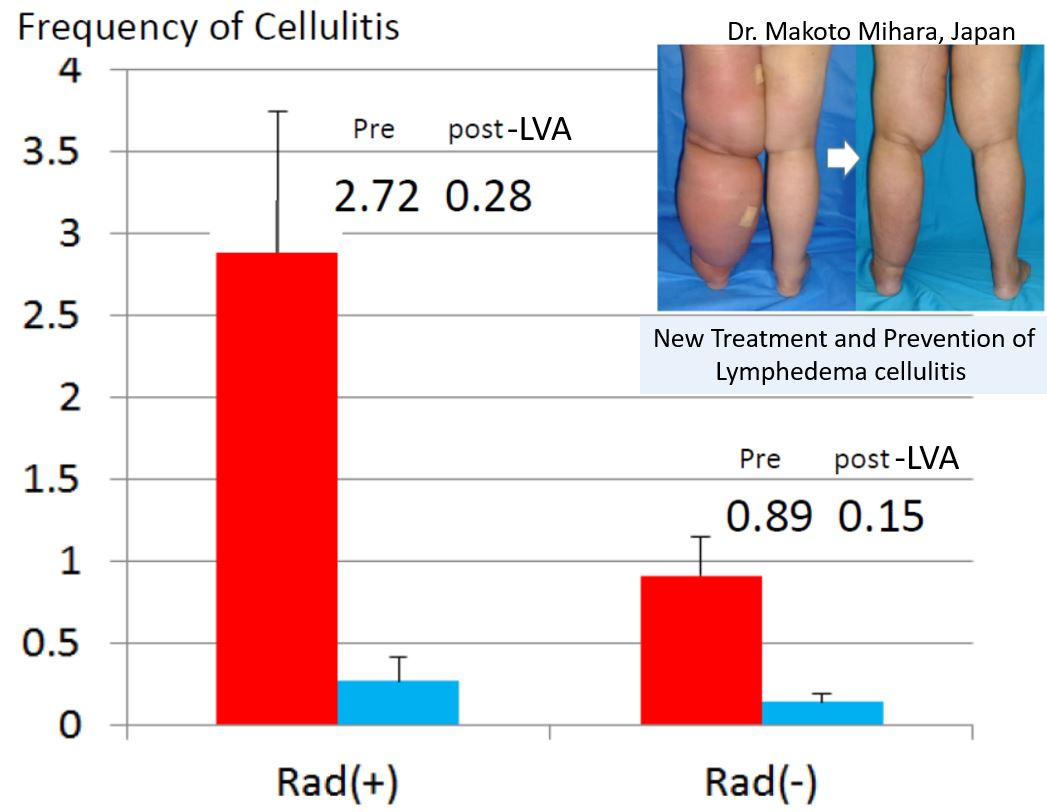
If cellulitis develops despite conservative therapy, surgery is recommended. Lymphatic venous anastomosis reduces the cellulitis rate to about one-eighth. In addition, even if cellulitis develops after this surgery, it is unusual for the fever to reach as high as 38-40℃, often remaining at about 37℃. If the patient rests well, sleeping through the night, symptoms are often markedly reduced the next morning, allowing the patient to carry out the activities of daily life.
The only prophylactic measures for cellulitis in use until now were physiotherapy and long-term oral antibiotic administration, but surgery has recently been accepted as an alternative. Please feel free to consult us or to ask questions about surgery, even if the issues seem small or unimportant.
If you have lymphatic vesicles in the genital region, bacteria can enter your body there, resulting in cellulitis. Treatment of lymphatic vesicles thus prevents the onset of cellulitis.
The most important issue is your current lymphatic function, and it is best for you first to undergo an examination by lymph scintigraphy.






Case study of a typical patient with lymphedema-complicating cellulitis
Numerous patients visit our clinic for treatment of lymphedema-complicating cellulitis by our medical team. If lymph scintigraphy confirms that there is residual lymphatic function, and it is judged that lymphatic venous anastomosis (LVA) is indicated, then surgery is recommended. This surgery has been shown to reduce the cellulitis rate in at least 95% of patients.
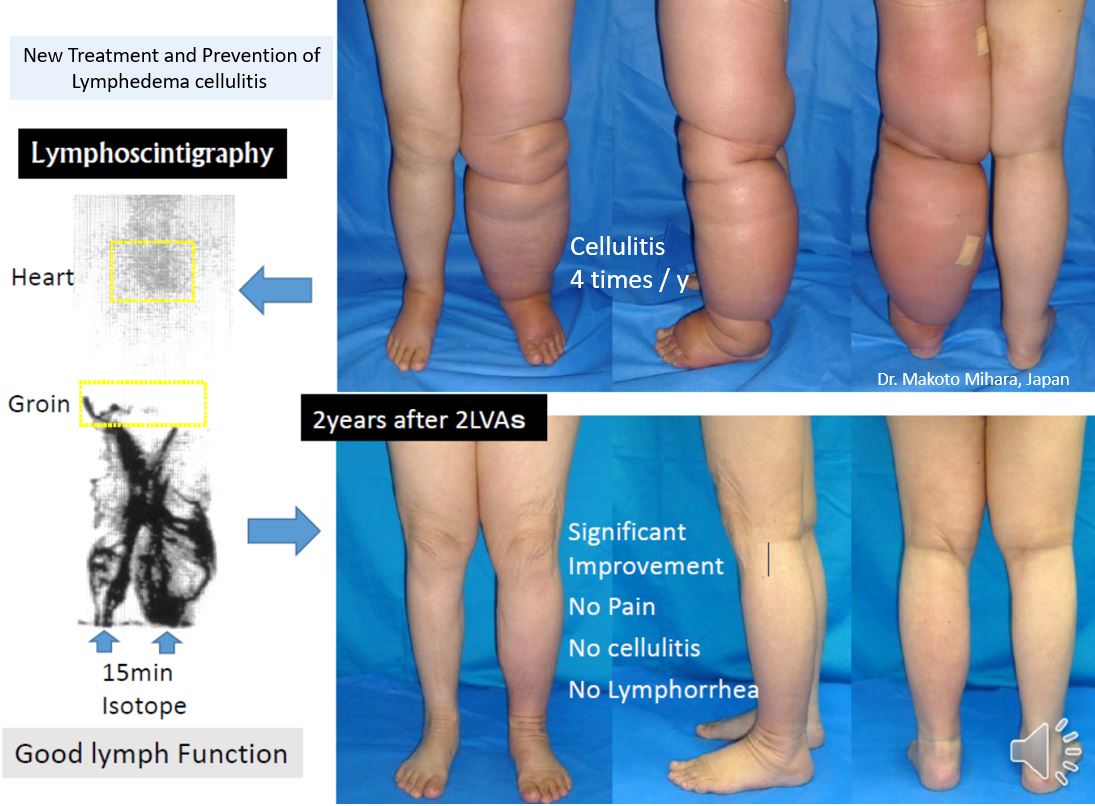
Our medical team previously treated a patient who arrived at the hospital complaining of the development of cellulitis as often as 20 times a year, but lymphatic venous anastomosis was performed twice, resulting in recovery, without even approximately one occurrence of cellulitis per year. The patient’s long-term postoperative outcome has been stable.

Treatment in Japan
If you have been given the appropriate conservative treatment in your own country, it will take about two weeks from your arrival in Japan to your return to your own country. This time includes diagnosis, and treatment (lymphatic venous anastomosis). If, on the other hand, you have not been given the appropriate conservative treatment in your own country, both conservative treatment and an LVA will be carried out here, and your estimated stay in Japan will be about four weeks.
The surgery itself will be carried out under local anesthetic. There have to date been no cases of postoperative complications such as irreversible nerve damage or bleeding. The annual rate of minor complications, such as lymphatic leakage from the affected area, is less than 1%. In the case of lymphatic leakage, full recovery is achieved gradually by a disinfectant treatment lasting about two weeks.
Before performing an LVA, our medical team will use lymph scintigraphy, indocyanine green lymphangiography, and/or ultrasonography to correctly identify the lymphatic vessel and vein to be operated on. Indocyanine green lymphangiography cannot be carried out with patients who are allergic to CT contrast agents, but the collecting lymphatic vessel can be identified correctly using ultrasonography for such patients. Due to the progress that has been made in these preoperative tests, the results of 10 conventional LVAs are comparable to those of 3 current LVAs, so it is now possible to provide treatment with higher success rates. We currently carry out LVAs on at least 400 limbs per year, which is the largest number for any clinic on the world.
Sicentific data about prevention cellulitis, 2024
In January 2024, our clinic reported new scientific evidence on the prevention of cellulitis in the British Journal of Surgery. We found that the combination of LVA surgery and conservative treatment was more effective at preventing cellulitis than conservative treatment alone. Click here for details of the paper.

Message from Dr. Makoto Mihara

Dear Patient,
Thank you very much for taking the time to learn about our clinic and our approach to lymphedema and recurrent cellulitis.
If you are reading this message, you may be living with lymphedema and experiencing repeated episodes of cellulitis, fever, or ongoing anxiety about your health.
Many of my patients tell us that the most difficult part is not only the physical symptoms, but also the constant fear of when the next episode might occur—especially when travel, work, or daily life feels uncertain.
I want you to know that you are not alone, and that these concerns are fully understood here.
At our clinic, we specialize in the comprehensive treatment of lymphedema.
We carefully combine conservative care, surgical treatment such as lymphaticovenular anastomosis (LVA), and thoughtful, time-limited use of medication—always guided by medical evidence and each patient’s individual condition.
For patients who live overseas, it is natural to feel anxious about:
・traveling to another country for medical care
・communication and follow-up after returning home
・what happens if fever or cellulitis occurs again
Because of this, we place great importance on continuity of care.
Even after online consultation or surgery, we provide free email-based follow-up support after you return to your home country.
If needed, we are also happy to collaborate with your local doctors or therapists so that your care continues smoothly.
Our goal is not simply to treat infection or perform surgery.
Our goal is to help you regain stability, confidence, and peace of mind—so that lymphedema and cellulitis no longer control your life.
Every patient’s condition is unique, and outcomes may vary.
However, I firmly believe that with careful evaluation, honest communication, and step-by-step treatment, meaningful improvement is possible for many patients.
If you have questions, concerns, or uncertainties—no matter how small they may seem—please do not hesitate to reach out.
We are here to listen, to explain, and to support you.
With my warmest regards,
Makoto Mihara, MD
Director, Lymphedema Clinic Tokyo, Japan
Scientific basis for this treatment
For scientific evidence, please refer to the following link:
We explain our published research papers and other world’s latest evidence-based lymphedema studies in a way that is easy for patients
to understand.
You can find these articles, along with patient-friendly summaries, at:
https://www.english-mominoki-shinryosho.net/research/
【Frequently Asked Questions (FAQ)】
About Scientific Evidence and Research Information
Q1. Where can I find scientific evidence supporting your treatment approach?
You can find the scientific evidence supporting our approach on the following page:
👉 https://www.english-mominoki-shinryosho.net/research/
On this page, we introduce our own published research papers as well as recent, high-quality international studies on lymphedema that we recommend.
Q2. Are these research articles written for medical professionals or patients?
The original research papers are written for medical professionals.
However, on our website, we provide patient-friendly explanations of these studies.
Our goal is to help patients understand:
what the research investigated
what the results mean in daily life
how the findings relate to treatment decisions
without requiring a medical background.
Q3. Why do you share research papers with patients?
We believe that patients should have access to transparent, evidence-based information.
By sharing and explaining scientific data, we aim to help you:
・understand the reasoning behind our treatment strategies
・feel confident in your medical decisions
・participate actively in your own care
We see research not as something distant, but as a tool to support patients.
Q4. Do these studies include only your clinic’s research?
No.
In addition to our own publications, we also introduce and explain important international research on lymphedema that we believe is valuable for patients.
These include studies from around the world that reflect the latest evidence and evolving understanding of lymphedema care.
Q5. Can I read these materials before deciding whether to visit your clinic?
Yes, absolutely.
Many international patients review these materials before online consultation or travel, as they help clarify expectations and treatment options.
We encourage you to explore the research page at your own pace and contact us if you have questions after reading.
Q6. What if I do not fully understand the research, even with explanations?
That is completely understandable.
Medical research can be complex.
If you have questions or would like clarification, please feel free to ask us.
We are always happy to explain the information in a way that makes sense to you.